LIE: "Studies show that opioids don't work for long-term chronic non cancer pain."
This article contains the following information:
- Introduction to the SPACE Trial
- Basic facts of the SPACE Trial
- Patients excluded from the SPACE Trial
- Bottom line results of the SPACE Trial
- Problems with Erin Krebs
- Problems or points of interest with the SPACE Trial
- Problems with how the SPACE Trial has been applied
- Examples of how media misrepresented the SPACE Trial
- Examples of how "medical experts" misapplied and misrepresented the SPACE Trial
- Quotes about the SPACE Trial from a variety of experts in different fields about the SPACE Trial
Introduction
When I first started researching this topic in 2017, I saw people saying "we don't have evidence showing opioids work for long-term chronic non cancer pain (LTCNCP)." Not long after that, I noticed they changed that statement to say "studies show opioids don't work for pain" That's a big difference. Lack of evidence that something works, isn't the same thing as evidence that it doesn't work. When asked to give the source for that claim, the study that's cited repeatedly is "The Strategies for Prescribing Analgesics Comparative Effectiveness, The SPACE Trial." It was a study published in JAMA in 2018 done by Dr. Erin Krebs, funded by the VA. Let's break down this study to show what it does and does not say. There is a lot of information here, with links to all of the sources. I highlighted parts that are extremely important.
The Study was done based on the following assumptions:
- "Long-term opioid therapy has been a common approach for managing moderate-severe chronic musculoskeletal pain."
- "Evidence for the effectiveness of opioid therapy for long term non cancer pain has been lacking (few studies last past 3 months)"
The goal of the study was: To have a Quality Random Controlled Trial (RCT) to evaluate the comparative long-term (>3-6 month) benefits and harms of opioids for low back pain, and osteoarthritis of hip and knee.
- It was a randomized trial
- It compared opioid therapy vs non-opioid therapy over 12 months for primary care patients with chronic back pain, hip or knee osteoarthritis pain of at least moderate severity.
- There were 240 patients in the trial.
- Mean age ~58
- 87% were male
- There was an opioid arm vs non-opioid arm
- There were 3 steps for the non-opioid arm
- Step 1: Acetaminophen and NSAID (like ibuprofen)
- Step 2: included adjuvant oral medications (ie, nortriptyline, amitriptyline, gabapentin) and topical analgesics (ie, capsaicin, lidocaine)
- Step 3 included drugs requiring prior authorization from the VA clinic (ie, pregabalin, duloxetine) and tramadol
- There were 3 steps for the opioid arm
- Step 1: Immediate release morphine, oxycodone, or hydrocodone
- Step 2: Morphine sustained-action Extended Release or Oxycodone Extended Release
- Step 3: Transdermal fentanyl
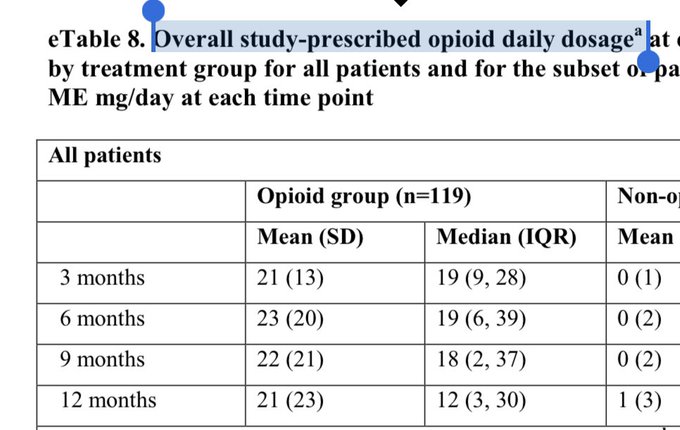
- Opioids were titrated to a maximum daily dosage of 100 morphine-equivalent (MME) average dose was 22 MME-(which is about 20 mg of Hydrocodone)-see chart below
- Follow-up visits were monthly until a stable regimen was established, then visits occurred every 1 to 3 months.
- Visits were in-person at 6 and 12 months when possible and otherwise mostly by telephone.
Here is a graphic posted by a chronic pain patient taken from the actual study showing the average MME (Milligram of Morphine Equivalent) dose (22 MME) for the opioid arm in the SPACE Trial
Those Excluded from the study:
- Those with high impact pain conditions (any condition other than low back pain and osteoarthritis (OA) of hip and knee)
- Patients on long-term opioid therapy
- Patients who were physically dependent on opioids
- Chronic pain patients
Bottom line of results:
- Showed that the non-opioid therapy group and opioid groups had similar results
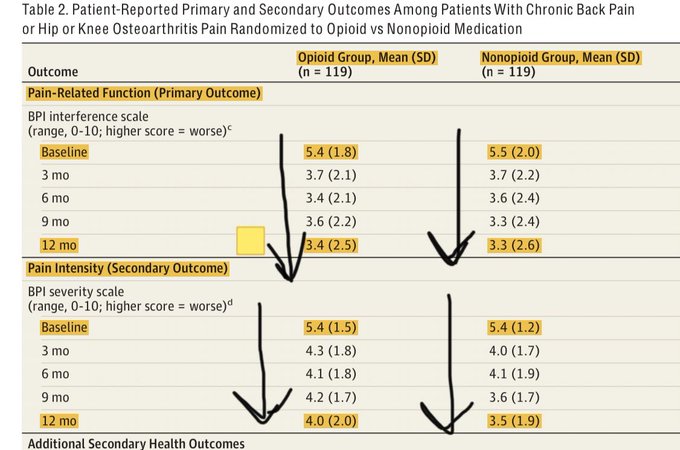
- Both groups had increased function and reduced pain. (See chart below showing this information)
- There was no significant difference in pain-related function between the 2 groups over 12 months.
- Pain intensity was slightly better in the non opioid group, but the clinical importance of this finding is unclear; the magnitude was small
- Health-related quality of life did not significantly differ between the 2 groups
- In this trial, pain-related function improved for most patients in each group
- Anxiety was significantly better in the opioid group
- There were no significant differences in adverse outcomes
- No significant difference in issues of misuse between the two groups
- No deaths, doctor-shopping, diversion or OUD were detected
Here is a graphic posted by Dr. Amaraqueye on Twitter showing how in both groups pain decreased and function increased
Problems with Erin Krebs herself (many of these points were made by Pat Anson from PNN in this article):
- She was already a well known anti-opioid zealot.
- She was on the Core Expert Group of the 2016 CDC Guidelines.
- She already had published anti-opioid propaganda.
- She was already a well known advocate of opioid tapering. In 2017 she reviewed 67 studies on opioid tapering. Regardless of the fact that the majority of the studies she reviewed were very low quality, she still came to a conclusion in favor of tapering
- Quote by Krebs about the review: “This review found insufficient evidence on adverse events related to opioid tapering, such as accidental overdose if patients resume use of high-dose opioids or switch to illicit opioid sources or onset of suicidality or other mental health symptoms.”
- Actual conclusion of the review itself: "Very low quality evidence suggests that several types of interventions may be effective to reduce or discontinue LTOT and that pain, function, and quality of life may improve with opioid dose reduction."
- Her work was praised by Andrew Kolodny, and has been cited to promote forced opioid tapering.
- As pointed out in the PNN article, Even Andrew Kolodny himself cited her review as a reason to force tapers by saying "dangerously high doses should be reduced even if patient refuses."
- Rummler Hope (fiscal sponsor of PROP) sponsored a talk she did called "Chronic Pain and Responsible Opioid Prescribing."
Problems or points of interest with the study:
- The average dose for the opioid group was 22 MME (around 20 mg Hydrocodone daily), which is outside typical therapeutic dose for someone with moderate to severe OA pain, yet the non opioid arm had high doses of acetaminophen, ibuprofen, as well as other meds like Cymbalta, Gabapentin, and Tramadol
-
Tramadol, an opioid, was used in the non-opioid arm of the study.
- The scope of the study was quite small, which in and of itself isn't a problem, if it weren't applied to those outside the scope of the study
- As stated above, CPP's other than with OA were excluded, and well as anyone on chronic opioid therapy, which is a problem because it's applied to all CPP's with all painful conditions
- Does not represent or apply to patients with a significant history of using opioids for CNCP, yet it is applied to all CPP's taking opioids
- Initial opioid limit was 200 MED/day; changed/reduced mid-study (so it's quite possible they didn't prescribe enough opioids for adequate pain relief, yet in the non opioid group, the medications were in high doses and many different meds were used)
- Of 4,485 with prior month health record of back or lower extremity pain, only 265 enrolled.1,843 declined to participate and 2,377 did not meet pain diagnosis and severity criteria (common exclusions: fibromyalgia, migraine, opioid or benzo use, mental health condition and substance use disorder).
Problems with how it's been applied:
- 87% were male, yet it is frequently used as a reason to force taper conditions specific to women like endometriosis
- They excluded chronic pain patients yet it's applied to all chronic pain conditions like Fibromyalgia, Lupus, Crohn's, and even Sickle Cell Disease
- They excluded those dependent on opioids yet it's applied to all dependent on opioids and used as a reason to force tapers
- Even though both groups had decreased pain and increased function, it's used to show that opioids don't work for pain yet it's also used to show OTC meds do work for pain
- The study chose chronic pain conditions that don't typically receive opioids for treatment, and then applied it to ALL chronic pain conditions
- SPACE Trial was misapplied by major publications claiming the study proves that opioids don't work for chronic pain.
- SPACE Trial showed few adverse outcomes in the opioid arm and zero cases of OUD, doctor-shopping, or death, yet it is repeatedly used to show that the risk of addiction is higher than we thought
- SPACE Trial was misapplied by "expert witnesses" such as Anna Lembke, and other "experts" such as Andrew Kolodny
- I've heard it said that Erin Krebs herself wasn't happy with how this was misapplied, but when asked about that, she didn't make that statement. From what I can tell, Dr. Krebs has never released a public statement warning about the misapplication of her study. I will include the citation and quote below.
Example of how media misrepresented the SPACE Trial:
Article in Vox "Finally Proof: Opioids Are No Better Than Other Medications For Some Chronic Pain": "Do opioids help patients with chronic pain in the long run? Are they worth all that risk? The answer, according , is a resounding “no.”'
Examples of how "medical experts" misapplied and misrepresented the SPACE Trial:
Lembke's testomony given under oath as an "expert witness" in opioid litigation in NY: "Researchers, including those who published an article in the Journal of the American Medical Association in 2018, were forced to conduct studies to counter the pharmaceutical companies’ opioid promotions. Those studies found that opioids were not effective for the long-term treatment of moderate to severe pain, and that the risk of addiction had been understated." Remember, neither statement is correct. SPACE Trial showed that opioids were effective AND showed that none of the 240 developed addiction, so show me how the results showed risk of addiction has been understated? This isn't the first time Lembke lied under oath. Remember the ruling by Judge Wilson in Ca that said her testimony was inaccurate and that she OVERSTATED the risk of addiction? I guess an "expert" would be willing to say just about anything in litigation if the pay rate were high enough. Anna Lembke has made millions as an expert witness in opioid litigation. She is a Psychiatrist, so she's not an expert in pain treatment, anyway. She testified in the same case that she makes $500-$800/hour as an expert witness. The article states "Dr. Anna Lembke acknowledged that she has been paid hundreds of thousands of dollars appearing as an expert witness for plaintiffs suing opioid makers in recent years."
Yet, any pain patient advocate is accused of being "industry funded." Dr. Lembke is funded by both the opioid elimination industry and the litigation industry.
Lembke said in an interview : “What I think is really important to remind people is that if opioids worked long-term, I would have no problem with patients taking them,” she said. “The fundamental issue is that they stop working and then you have an additional problem.” So, I guess she wouldn't have a problem with low back pain, OA of hip and knee patients taking opioids because the SPACE Trial shows they both decrease pain and increase function.Quote from Chou when asked about The SPACE Trial: "I think this is going to shake things up,” Roger Chou, a professor at Oregon Health and Science University who was not involved in the research. “The belief has always been opioids are the most effective pain medicine, certainly for acute pain and even for chronic pain. This [study] turns that on the head.”
Here is a presentation by CHOU that includes the SPACE Trial
Quote from Krebs when asked about the misapplication of The SPACE TRIAL: "My experience with advocates criticizing SPACE is similar to what I experienced when I participated in the 2016 CDC opioid prescribing guideline development process. In both cases, social media and internet-based criticism focused on claims that the work was biased and therefore illegitimate. I suspect this type of criticism is fueled less by misleading media reports than by misleading industry-supported advocacy." It doesn't sound to me like she wanted to take that moment to express concern about the misapplication. Instead, she did just what Kolodny does, and instead of commenting on the actual issue, she accuses those with concerns of being industry funded.
Quote from Krebs when asked about the influence of the SPACE Trial: Although it's a bit too early for our study findings to be incorporated into guidelines, I have heard from many individual clinicians that this study has influenced their clinical practice and teaching of trainees. I expect our results to be interpreted as providing support for recent guideline recommendations. The 2016 Centers for Disease Control and Prevention opioid guideline advised that non-drug therapies and non-opioid medications are preferred for chronic pain, and the 2017 VA opioid guideline advised against starting long-term opioids for chronic pain. These recommendations were based on expert opinion and data about opioid-related harms. Our study contributes long-term evidence on the benefit side of the equation—we found no advantages to opioids that would outweigh their greater risk of serious harm. The results should reassure clinicians that following current guidelines is not likely to result in undertreatment of pain." Huh, interesting considering her study is cited as reasons to force taper, not treat acute post-op pain, and to deny opioids for all severe chronic pain conditions.
A newsletter put out by Health Professionals for Proper Opioid Prescribing (PROP) stated: "The best evidence now shows that prescription opioids are ineffective for long-term management of common chronic pain conditions, such as osteoarthritis and low back pain. Reducing opioid use for acute pain (after injuries, post-op) leads to fewer persons transitioning to chronic opioids, fewer then becoming opioid-dependent, fewer persons becoming addicted, and ultimately fewer opioid overdose deaths." Again, this is false. The study didn't show opioids are ineffective.
Here are some quotes from experts in different fields, a pain/addiction doctor, a PharmD, a Psychologist, a Researcher, a civil rights lawyer:
Quote on Twitter from Dr. Stefan Kertesz: "Among patients who volunteered to be randomized to 2 treatments that usually have only modest benefits, both groups improved to a larger-than-expected degree, with the apparent improvement in status persisting a year. Adverse effects that are expected & typical, proved rare. "
Quote on Twitter from Dr. Amarquaye: "They even showed both decrease in pain related function and intensity in both the opioid and non opioid group at 12 months."
Quotes on Twitter from Dr. Michael Schatman: "To call the SPACE study "the best evidence" against prescription opioids for chronic pain is laughable, demonstrating a horrific misapplication of junk science. Thanks for posting. You'll soon be reading a robust responding editorial regarding your false claims."
Quote on Twitter from Kate Nicholson, a lawyer and CPP: "it is one study of mostly moderate severity orthopedic and arthritic pain. Grouping all types and severities of chronic pain together to suggest as 60 Minutes did that there is something illegitimate about the use of opioids for all long-term pain is problematic."
Quote by Red Lawhern, Researcher:'The SPACE study was flawed by selection of patients who would normally not be candidates for opioid therapy, and titrating these patients very rapidly. Likewise, is Tramadol a non-opioid? That's the way it was labeled.'
Read this article in PNN called "Is JAMA Opioid Study Based on Junk Science?"
There have been some reviews of studies of opioids for long term non cancer pain. They are generally discounted to to being weak evidence, which I find odd since the entire CDC Guidelines were based on a similar review of studies by actually the same author also showing weak evidence. Hypocritical? Or just more proof that all of this was done for their litigation narrative?
This content was written by Bev Schechtman and Carrie Judy for The Doctor Patient Forum.