







PharmedOut is an organization started with a grant from the Attorneys General. This grant came from settlement funds from litigation against Pfizer for marketing their medication, Neurontin, off-label. $325,000,000 was made all together, and Adriane Fugh-Berman was given a $400,000 grant to start PharmedOut. PharmedOut recently sent an e-mail with updates. Their mission is one I mostly agree with: "To investigate the influence of pharmaceutical industry marketing on the practice of medicine; foster access to unbiased information on drugs; and create and promote pharma-free continuing medical education to providers." The problem I have with them is it seems as though most of their advocacy work has been about opioid prescribing and chronic pain patients. Oh, and she has made quite a bit of money as an expert witness in litigation. Sure seems like the AG's gave her money from litigation settlement in order to start an organization that can bring in more litigation settlement funds. Round and round it goes. Oh, and Fugh-Berman is a founding member of PROP.
Fugh-Berman is debating Jeffrey Singer on June 7, 2022. You can purchase tickets here. Kolodny was originally set to debate Dr. Singer, but has backed out for unknown reasons. Undoubtedly, Fugh-Berman will claim Singer is "industry funded," as they do anyone who dares to disagree with them.
Pharmed Out's recent e-mail included content from Judy Butler, a fellow with PROP and PharmedOut. Like always, they focus on CPP's and "industry funding." They take a little truth and twist it to present an argument that is both false and misleading. The rest of this article will be breaking down Butler's e-mail comment by comment. Their statements will be in black and our responses in blue.
Let's lose the term "legitimate pain patient"
by Judy Butler
PharmedOut: "The frame of good versus bad opioid users, seen over and over, again made recent news. This month the Supreme Court heard arguments addressing a “good faith” defense in criminal cases involving the prescribing of opioids. Under the Controlled Substances Act (CSA), an authorized prescriber can dispense these drugs “for a legitimate medical purpose“ when “acting in the usual course of his professional practice.” Pain patient advocates argue that prescribers should not be criminally liable unless they intend to prescribe without a legitimate medical purpose. They reason that fear of criminal prosecution deters prescribers from using their best medical judgment to treat pain. With opioids, of course."
The Doctor Patient Forum: The Supreme Court did recently hear a case about Dr. Ruan. He wasn't given the opportunity to use a good faith clause defense, so it was heard before the Supreme Court. We covered the Ruan case in detail. She's right. Fear of criminal prosecution does deter prescribers from prescribing. Why would they feel comfortable prescribing if they feel they don't have any protection?
Pharmed Out: "This case comes on the heels of the release of the CDC’s draft Clinical Practice Guideline for Prescribing Opioids, which updates and expands upon their 2016 Guideline. Most notably, the new recommendations no longer include suggested limits on the dose and duration of opioid prescriptions."
The Doctor Patient Forum: This part is true. The CDC is updating/expanding their opioid prescribing guidelines. Read our article about how to comment on the new CDC Guidelines. You have until April 11, 2022.The CDC has finally acknowledged harm done by arbitrary thresholds and have created a draft that excluded these MME and day limits in the main recommendations. These arbitrary thresholds are still included in the supporting text of the draft.
PharmedOut: "Predictably, pain patient advocates framed the revisions as a win because the opioids-for-pain advocates push back on any and all measures to curtail opioid overprescribing."
The Doctor Patient Forum: Yes, we have tentatively framed the revisions as a win, but not due to the reason she gives. We don't push back on "any and all measures to curtail opioid prescribing." We push back because the CDC Guidelines have led to mass harm including untreated pain, suicides, overdoses, and mental health crises. Dr. Kertesz is currently running a study about suicides associated with force tapers or reductions of opioids. Check out the following video of Dr. Kertesz presenting his study before colleagues. Fugh-Berman pushed back making claims that this study isn't really necessary. Can you imagine? A doctor pushing back on a study about suicide? Why would this be? Could it be because they don't want the truth out there of the harms done to CPP's by a false narrative they help promote? Listen to more from Dr. Kertesz on his podcast.
Fugh-Berman pushing back about Dr. Kertesz' study on suicides:
PharmedOut: "The unstated message is that any “legitimate pain patient” may benefit from opioid treatment. They argue that because “legitimate pain patients” don’t divert drugs, and, somehow, are magically protected from misuse, their unimpeded access to opioids must be protected."
The Doctor Patient Forum: How does she know what our "unstated message" is if it's not stated? I've actually not seen CPP's or CPP advocacy orgs claim "legitimate pain patients" have never diverted drugs and are "somehow magically protected from misuse," leading us to want "unimpeded access to opioids." This is how they twist the truth. What we DO claim is the actual statistics about CPP's and addiction are not even close to what they claim. We have a table of recent statistics available for you. See the difference? We say: studies show 1-5% of CPP's may develop addiction. They say: "CPP's claim they are magically protected from addiction." We say: "Our doctors should be free to prescribe opioids as they see fit." They say: "CPP's want unimpeded access to opioids."
PharmedOut: "This decades-old delineation between “legitimate pain patients” and abusers is a marketing message, created by Purdue Pharma in response to the worrisome rise in opioid addiction seen after the introduction of OxyContin. As Richard Sackler put it – “we have to hammer on the abusers in every way possible. They are the culprits and the problem.”
The Doctor Patient Forum: Actually the DEA is who came up with the campaign called "Good Medicine Bad Behavior." Did Richard Sackler say that? Very possible, but I'm struggling to see how a marketing technique used by Purdue over 2 decades ago has anything to do with CPP's begging for access to prescription opioids. CPP's aren't begging for access to pain meds because Arthur Sackler convinced us or our doctors that opioids work for pain. We are fighting for access because opioids have helped our pain. Andrew Kolodny claimed CPP's and people with OUD are one group, how we can't think of ourselves as separate. CPP's and CPP advocacy orgs wouldn't have to try to separate the groups if Kolodny didn't create the false narrative that we are one in the same. Both groups deserve compassion and access to treatment, but that doesn't mean that we are the same as far as types of treatment or diagnosis. I don't like the term "legitimate pain patients" either, actually. It makes it sound like we have to prove we are in pain, and that there are a group of CPP's that "aren't legitimate." But, that's not the point she's making. She's saying that we claim we are "legitimate" pain patients because we want to "hammer the abusers." This is false. We support those with OUD, and fight for their rights, also. This push to pit one group against the other was a technique started early on by those who had their eyes on opioid litigation. Stop treating all CPP's like we are all liars and manipulators, and we will stop using the term "legitimate pain patients."
PharmedOut: "Arguing that opioid prescribing decisions should be left to the best medical judgment of doctors with good intentions sounds deceptively reasonable, but it won’t address the complex problems resulting from decades of overprescribing. In fact, it will make them worse."
The Doctor Patient Forum: Asking that doctors be allowed to decide what their patients should be prescribed has nothing to do with "decades of overprescribing." True "pill mills" weren't really a case of overprescribing. Many weren't doctors who were trying to help their patients. Many were drug dealers. But, these pill mills are a thing of the past. The DEA moved on from targeting what they thought were true pill mills to targeting doctors who are prescribing reasonably. This has caused doctors to fear the DEA or their medical board and stop prescribing and/or dismiss CPP's from their practice. I'd love to ask Ms. Butler if she's advocating for doctors to not make medical decisions based on their judgment, what should it be based on? CDC Guidelines? The government? Rummler Hope? Shatterproof? Well, we've tried that experiment. That is the cause of the mess we are now in that has contributed to over 100,000 deaths. We have 30+ states that have made laws based on non evidence based CDC Guidelines, and we have doctors sitting in prison simply for treating pain and anxiety.
PharmedOut: "Aggressive opioid promotion has long-lasting effects that are difficult to reverse. Opioid prescribing rates remain significantly higher than before the opioid crisis..."
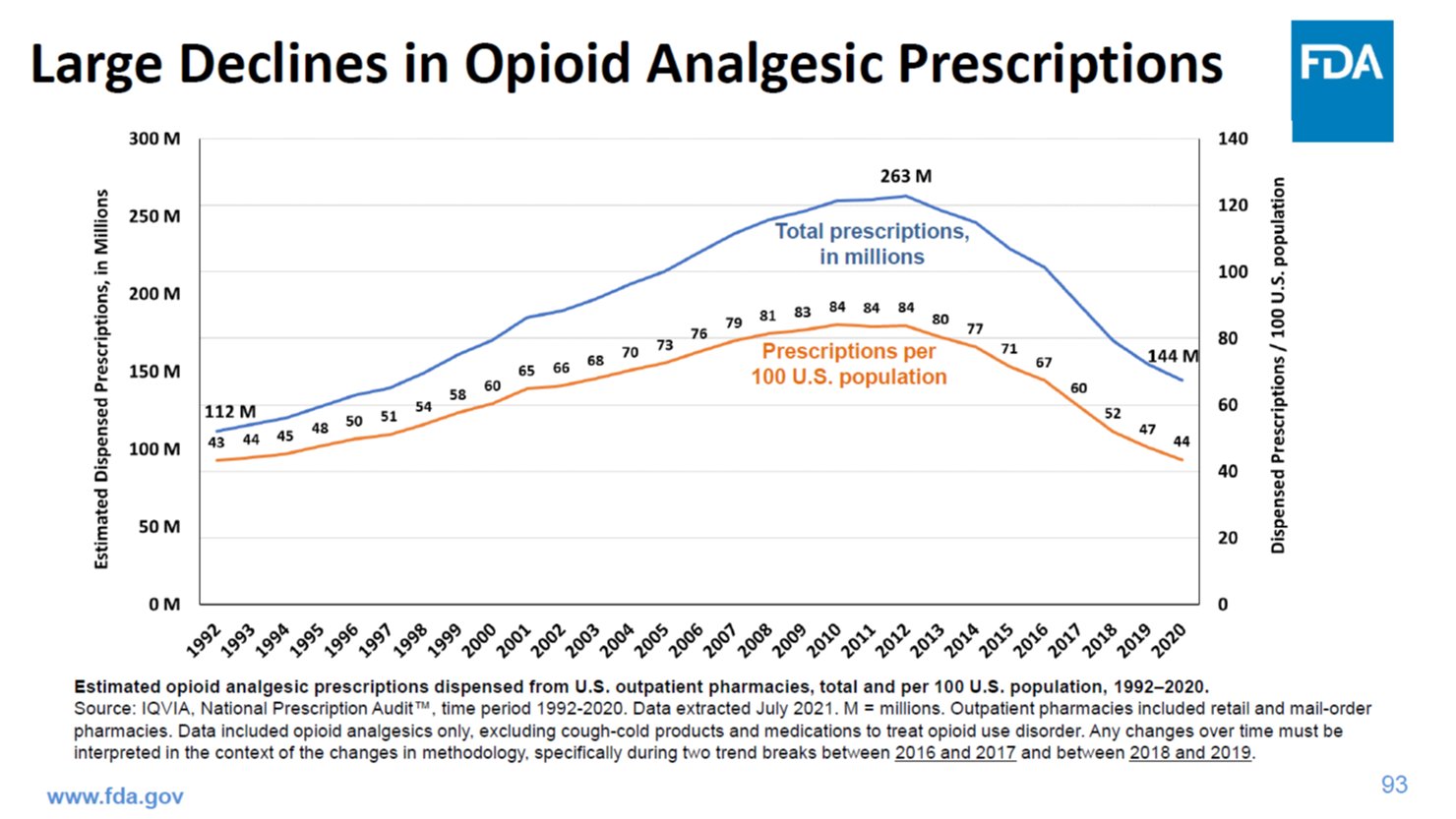
The Doctor Patient Forum: This is 100% false. I'll give her the benefit of the doubt and say she's uniformed and not spreading false information on purpose. Prescribing is actually down to the level of 1993, before OxyContin was even approved. Even if the claim is correct that there was a wave in prescription opioid deaths starting in around 1999, that still doesn't substantiate the claim that "opioid prescribing rates remain significantly higher than before the opioid crisis." How about you give out accurate information, PharmedOut? Considering you claim to promote transparency and facts, I'd imagine you'd want to put out facts instead of lies. Unless you're saying the "opioid crisis" started prior to 1993, in which case you should clarify.
PharmedOut:.."and industry payments to doctors continue to be associated with increased prescribing. Industry-aligned groups continue to challenge effective public health measures aimed at reining in overprescribing."
The Doctor Patient Forum: I've looked up the doctors who are the most vocal in support of CPP's. I don't see any of them taking money from opioid manufacturers. Check it out for yourself on Dollars for Docs or OpenPayments.com. As far as advocacy groups, I can only speak about those I know. The Doctor Patient Forum has never taken a penny from any industry. Ever. Try again. But, I would say that it's a fact that some of the most vocal anti-opioid zealots like Gary Mendell with Shatterproof, have taken a pretty penny from industry. They have taken from Pacira, Indivior, Alkermes, Adapt, Braeburn, and I'm sure I'm missing some. Indivior makes Suboxone, which is an opioid. 2017 is the only year they have their donors listed, so I can't speak to other years. Kolodny is on their board, though. So, apparently he's ok with industry funded addiction orgs. Rummler Hope, which Kolodny is also on the board of, claims they don't take from industry. I wouldn't know if this is true or not, because they never list their donors. You may be wondering if PROP takes money from industry. Nobody knows. Rummler Hope is the fiscal sponsor of PROP, so nobody knows anything about their funding at all. Pretty shady, if you ask me. So much for transparency, right Ms. Fugh-Berman? Since you're listed on their board of directors and you claim to fight for transparency, how about you ask PROP to be transparent also? Why the need to hide donors? While I'm at it, does PharmedOut actually list their donors? Maybe I'm missing them, but I can't seem to find them on your website.
PharmedOut: "Perhaps most significantly, a generation of patients have been prescribed long-term opioids for chronic pain – in the absence of any evidence that it works."
The Doctor Patient Forum: Actually, there is evidence that opioids work for long-term chronic pain. You and the rest of the anti-opioid zealots have determined in your infinite wisdom that it doesn't count as evidence because it's not randomly controlled trials. Cochrane review studies show some benefit from opioids. For the CDC Guidelines, they refused to accept any studies that were 3 months long or less, and there weren't really long-term studies done. So, therefore, they claim no evidence. There was one study, The Space Trial, which actually has been horrifyingly misapplied, that does also show some reduced pain and increased function for low back, hip, and knee arthritic pain patients. But, instead this study is used as a weapon to not prescribe and to force taper all CPP's.
PharmedOut: "In fact, in recent years, it has become clear that opioids are ineffective for chronic pain,..."
The Doctor Patient Forum: See what they did? They moved from "there isn't evidence to show that opioids work for long-term chronic pain" to "it has become clear that opioids are ineffective for chronic pain." This statement is false. The same lack of studies they cite showing opioids work are the same lack of studies showing opioids don't work.
Pharmed Out: "...can even worsen pain, and are dangerous to use long-term."
The Doctor Patient Forum: They're referring to Opioid Induced Hyperalgesia, which has never been proven in humans. It has been shown in studies in rats. It has maybe been observed by some doctors, but the cause hasn't been determined. We explained this in depth in our debunking lies section. As far as a blanket statement that opioids are dangerous to use long-term, it's misleading and inaccurate. Opioids being dangerous isn't a linear concept. Many things go into determining this such as age, comorbidities, other meds someone is taking, among many other things. They make this statement to sound like long term opioids are dangerous for everyone all the time. They love to speak in absolutes to mislead their readers.
PharmedOut: "The treatment of pain patients dependent on opioids, including opioid tapering, is a long-term, complicated process. Only a reduction in overprescribing will save a new generation from the same fate."
The Doctor Patient Forum: We agree that treatment of CPP's can be complicated. Tapering should be individualized and never forced on the patient. As far as the comment about reduction in overprescribing saving a new generation from the same fate...again, prescribing is down to the level of 1993, years before OxyContin was approved. How much lower do they want to go? When will it be low enough? This is also why they love to refer to us as the "lost generation." No stigma there, right?
PharmedOut: "Patients on long-term opioids absolutely deserve care, and that care includes continuing opioids at least temporarily. Care also means medical support for tapers (when appropriate, which it usually is)..."
The Doctor Patient Forum: I'm happy to hear they acknowledge that patients on long-term opioids deserve care. I object to the fact they claim tapering is usually appropriate. Judy Butler isn't a doctor, in fact I don't know what her credentials are other than she's a fellow with PROP and PharmedOut. I haven't seen studies showing most CPP's should be force tapered (other than statements by PROP members like Jane Ballantyne), but I have seen significant information from true "tapering" experts claiming nobody should be force tapered unless there are specific circumstances. The harm that has occurred due to medical abandonment of CPP's and force tapers or even stopping prescriptions cold turkey is increasingly being discussed. Finally.
PharmedOut: "...(care also means) advocating for coverage of effective non-opioid treatments, and support for research on pain that is not funded by pharmaceutical companies."
The Doctor Patient Forum: Coverage of effective non-opioid treatments would be amazing in addiction to access to prescription opioids when appropriate. I'd personally love to go to physical therapy weekly, but it's only partially covered. Unfortunately, some of the things they're calling effective don't work for many and haven't been sufficiently studied. The same things they tend to call "pseudoscience" when offered for those with addiction, they call "evidence based" when talking about pain. Things like tai chi and mindfulness. Again, if offered with the option of opioids when needed, I have no problem with them. We always agree with a multimodal approach, but these days that usually means all modes except opioids. As far as "research not funded by pharmaceutical companies," they need to attack the whole system, then. This is how our system works. Studies for Suboxone are often funded by Indivior, studies for Spinal Cord Stimulators are often funded by the companies that make them. To make it sound like opioids manufacturers are the only pharma that does this is misleading. I'd love to add to that statement, that this research also shouldn't be funded by pharma that benefits from opioid elimination. This research should also not be funded by litigation funds or lawyers or orgs that benefit from litigation. This is an "industry funding" that is hardly ever mentioned.
PharmedOut: "Unrestrained access to opioids is not good medical care."
The Doctor Patient Forum: Nobody is claiming it is. If a CPP or CPP org claims that opioids should be available as an option that doesn't mean we are advocating for unrestrained access to opioids. Yet, this is always the way they present it. We are advocating for balanced pain care where our doctors have the option to try opioids without fear of the DEA or their medical board.
PharmedOut: "Opioid manufacturers told physicians that opioids were good for arthritis, low back pain, and headaches: conditions that opioids should never be used for."
The Doctor Patient Forum: What opioid manufacturers told physicians about opioids shouldn't affect adequate pain treatment. This is what anti-opioid zealots do. They claim pharma lied and therefore patients should be punished. It is false that opioids should "never" be used for these conditions. Again, why the need to speak in absolutes? Why is Judy Butler, who isn't a pain doctor, making claims in absolutes about what should and shouldn't be treated with opioids? If you look at content from actual experts in these conditions, they seem to agree that opioids shouldn't be the FIRST line of treatment for them. There is a huge difference between stating that and stating that opioids should never be used for these conditions.
PharmedOut: "Corporate “educational” efforts over decades may have persuaded many physicians that opioids are reasonable treatments for ordinary pain syndromes, but believing doesn’t make it so.
The Doctor Patient Forum: Again, what does corporate's educational efforts have to do with anything? I'll make a similar claim about Ms. Butler; corporate educational efforts may have persuaded many physicians that opioids are NEVER reasonable treatment for just about anything, but believing doesn't make it so. If there was opioid prescribing that was too liberal, creating a climate where there is very little opioid prescribing doesn't fix things, it just causes a different set of issues. Hence the untreated pain crisis along with the illicit fentanyl poisoning crisis.
PharmedOut: "Pain doesn’t protect patients from opioid use disorder and addiction, which can wreck lives and kill people."
The Doctor Patient Forum: Who is making that claim? Maybe certain pharma did decades ago, but I'd like to see one pain doctor or expert making that claim now. This is one of their techniques they love to use. They argue points that may have been applicable 20 years ago and act as if this is taking place today. Nobody is saying CPP's can't have OUD, in fact there are some who do, but CPP's with OUD deserve compassionate pain care, also.
PharmedOut: "There’s a reason opioids are controlled substances: they’re addictive."
The Doctor Patient Forum: Who is making the claim that opioids don't have the potential to be addictive? I haven't seen anyone say this.
PharmedOut: "Prescribers with good intentions to treat pain got a pass when they were duped by industry misinformation about addiction that influenced medical practice."
The Doctor Patient Forum: Prescribers didn't get a pass. At all. Many doctors are in prison. Many doctors stopped prescribing because they're scared of going to prison. Who is it that got a pass?
PharmedOut: "Giving a pass to prescribers who intend to treat chronic pain with opioids means giving a pass for overprescribing.
The Doctor Patient Forum: Read that statement closely. So if a prescriber gives opioids intending to treat chronic pain, that means that doctor is overprescribing? So, that sounds like no chronic pain patients should get opioids. What exactly is the definition of "overprescribing"? Seems like Ms. Butler is implying that any opioid prescribing for chronic pain is overprescribing. Which is exactly what they seem to teach.
PharmedOut: "Restrictions on opioid prescribing save lives."
The Doctor Patient Forum: Here is another claim with zero evidence. Let's look at the number of drug deaths there were when PROP got started compared to now. Around 15,000 then and over 100,000 now. I'd make the claim that restrictions on opioid prescribing actually causes deaths. We don't have proof of that quite yet, but I hope someone studies this soon. The only reason we don't have evidence of patient outcome from bad prescribing policy is because nobody seems to want to measure patient outcome. The only metric that matters is level of prescribing. So, prescribing is down, therefore they claim success. We have heard quite a bit of anecdotal evidence of CPP's being denied opioids then either committing suicide or obtaining their medication elsewhere. We have had at least one CPP in our organization who was denied meds and then died after going to the street for medication to try to treat her pain.