Bev's story about being denied opioids due to having been sexually abused
In November 2017, I (Bev) did something I had done many times before; I went to the emergency room due to kidney stone pain. I had frequent kidney stones due to having Crohn's Disease. Although I had pain medication at home, I was unable to keep it down, and the pain was unbearable. My doctors had always told me if I couldn't take the pain or couldn't stop vomiting, to go to the emergency room. Recent scans showed multiple kidney stones in the ureters. The ER doctor was kind; she treated my pain and decided to admit me for pain control. That's when things took a turn. Upon entering the room, the hospitalist said "I saw in your prescription history that you have gotten Ativan, What was that for?" I told him it had nothing to do with why I was there, that it was for PTSD. The rest of the conversation went like this: Dr.: "What is your PTSD from?" Me: "Childhood trauma." Dr.: "What kind of childhood trauma?" Me: "I don't understand why this matters." Dr. "Was it from sexual abuse?" Me: "Yes." Dr. "Due to that, I can't give you any IV opioids. I can give you what you take at home, and I'll give you a bit of a higher dose, but you're too high risk of addiction because you were sexually abused as a child." I was shocked and mortified. He then said "IV opioids change your brain chemistry and so does sexual abuse. You have a high risk of addiction and I won't take part in causing that." He then hit me on the arm and said:
"You'll thank me someday for this."
I was then treated horribly for the next 24 hours until I went home. It was from that hospital bed that I first contacted Claudia, and why I started researching and advocating. I had never had childhood abuse used against me in health care. Nobody had ever asked me this question before, and never in my wildest dreams (or worse nightmare) did I think this doctor would use this information to deny pain medication. While researching North Carolina's pain guidance from the medical board, I came across the information about the Opioid Risk Tool (ORT). Their information told doctors to give all patients the ORT before giving opioids.
This was in 2017 and it still affects me. It traumatized me. I'm terrified to ever go to the hospital again. I'm afraid of doctors. I can't express strongly enough how much this one incident changed my life. It damaged me. I'm fighting back and hoping to be a voice to others who this has happened to.
Maia Szalavitz discussed my story in the Wired article "The Pain Was Unbearable So Why Did Doctors Turn Her Away."
What is the ORT?
The ORT is a risk mitigation tool, meant to see who may be high risk for addiction so the doctor can keep a close watch on those patients. It was created in 2005 from Dr. Lynn Webster.
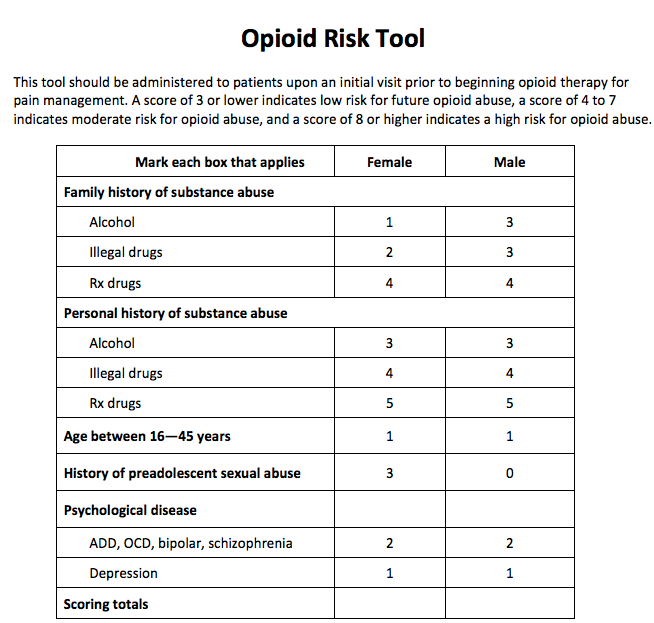
The first thing I noticed was that when a woman answers yes to the sexual abuse question, she's given 3 points against her. Yet, a man gets 0 points. This was done because the study used as evidence for this question was one that only researched the connection of women sexual abuse survivors and addiction. Little did I know that I wasn't the only person this happened to. For the past few years, I've gotten quite a few stories from women who had been sexually abused, assaulted, or even physically abused that had a doctor use that information as a reason to deny opioids
Dr. Webster's statement about the ORT being weaponized
In 2019 Claudia interviewed Dr. Lynn Webster and I called in to talk to him. I told him what happened and he said that was a weaponization of the tool, and it shouldn't be used that way. He then wrote about the weaponization of the ORT in an article in Pain News Network "The Opioid Risk Tool Has Been Weaponized Against Pain Patients."
It is a cruel misapplication of the ORT to use a background of sexual abuse as the only criterion to assess whether a patient should receive opioid therapy. The ORT is an important tool in mitigating harm that prescribing opioids could cause. It should not be weaponized to justify denying people in pain appropriate therapy.
Unfortunately, this didn't help the situation. We've continued to hear from women who were denied opioids due to being a survivor of sexual abuse/assault. Has the ORT been worked into risk score algorithms like NarxCare? Nobody knows for sure since their algorithm is proprietary, but I would say probably. We do know it's been embedded in EHR (Electronic Health Record) CDS (Clinical Decision Support Tools). I was left with the question of how do we fix this.
Study validating ORT/Updated version eliminating the sexual abuse question
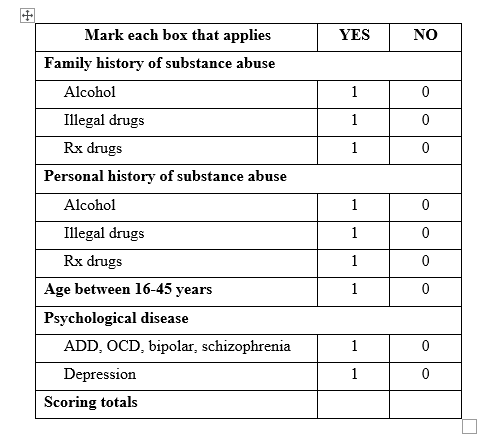
Carrie Judy, our other researcher, while researching ORT came across a relatively new study from 2019 by Dr. Martin Cheatle. This study's purpose was to validate the ORT. The results showed that the sexual abuse question wasn't relevant, and that the ORT was actually more reliable when removing that question. He created an updated version of the ORT leaving the sexual abuse question off.
Listen to Dr. Cheatle discuss why the sexual abuse question should be removed:
We got a lot of feedback that female patients didn't want to answer that question; it caused too much trauma
Unfortunately, there hasn’t appeared to be any formal effort to make sure the original ORT would be replaced by the updated version. As we stated, we are aware the ORT has been embedded in some Electronic Health Record platforms and also worked into some risk scores. It’s given by doctors and treatment centers, Since some risk scores such as NarxCare are proprietary, there is no way to know if the ORT is used in their algorithm, and if so which version.
ORT_letter_Final_version_for_website.docx
Dr. Webster says the original ORT should no longer be used
Periodically over the years we've asked Dr. Webster to release a statement for agencies and doctors to use the updated version instead of the original. On June 29, 2022 he listened and wrote “Another Look at the Opioid Risk Tool.”
It distresses me to know that, while the original ORT served to help assess the risk opioids posed for individuals, it has also caused harm. Since the question about a woman's sexual abuse history does not provide any additional benefit, there is no reason to retain it. The revised ORT should be used instead of the original ORT.
What Can You Do to Help?
We have noticed that most government agencies, individual doctors, and treatment centers still use the original version of the ORT. We plan to create an open letter (and will post it here) to formally request places that use the original to replace it with the updated version.
If you're given the ORT, please check to see which version it is. If the sexual abuse question is included, please show your doctor this information and explain that evidence shows the updated version is superior, and that the creator of the ORT released a statement to not use the original version.
Here is a letter (pdf) (Word) you can show your doctor that includes all of this information.
If you've been denied opioids due to being a survivor of abuse, please contact me at bevschecht@icloud.com.







